[4] Common sedative agents used during rapid sequence intubation
Do they sedate you before intubation?
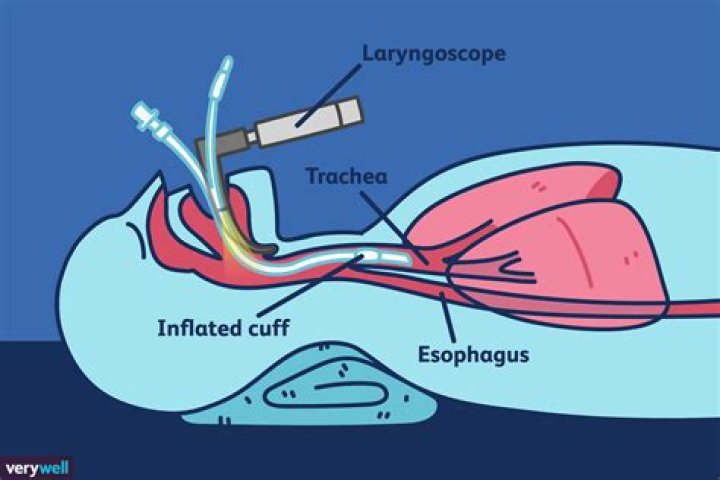
Unless the patient is already unconscious or if there is a rare medical reason to avoid sedation, patients are typically sedated for intubation. Intubation is a medical procedure used by doctors to keep the airway open or safe during a medical emergency or a surgical procedure.
What anesthesia is required for intubation?
General Anesthesia This type of anesthesia may inhibit or stop your breathing and may requires intubation (placement of a breathing tube), or placement of an airway device to assist with breathing.
What drugs are used with ventilators?
Propofol (P) and midazolam (M) are frequently given by continuous infusion for sedation in critically ill, mechanically ventilated patients.What muscle relaxant is used for intubation?
Muscle relaxants are given as part of a rapid-sequence induction to facilitate tracheal intubation. Among all the muscle relaxants available, succinylcholine is the only one with a fast (approximately equal to 1 min) onset and a fast recovery.
What is the difference between a ventilator and a respirator?
Your doctor might call it a “mechanical ventilator.” People also often refer to it as a “breathing machine” or “respirator.” Technically, a respirator is a mask that medical workers wear when they care for someone with a contagious illness. A ventilator is a bedside machine with tubes that connect to your airways.
Is intubation the same as life support?
“Intubating a patient and putting them on a ventilator to help them breathe definitely means they are being put on life support, which is very scary to think about when it’s you or your loved one needing that treatment.”
What is propofol used for in ICU?
PROPOFOL is an intravenous sedative–hypnotic agent that is commonly administered for sedation of patients in the intensive care unit (ICU) who are being treated with tracheal intubation and mechanical ventilation.Why is propofol used for mechanical ventilation?
Propofol has a number of properties that make it a potentially superior choice for sedation of intubated ICU patients. The rapid onset and offset of sedation with propofol, even after prolonged administration, allow for greater control over the level of sedation and more rapid weaning from mechanical ventilation.
What are the side effects of taking Remdesivir?- severe headache, pounding in your neck or ears;
- fast, slow, or pounding heartbeats;
- wheezing, trouble breathing;
- swelling in your face;
- nausea;
- fever, chills, or shivering;
- itching, sweating; or.
- a light-headed feeling, like you might pass out;
Is intubation the same as ventilator?
Intubation is placing a tube in your throat to help move air in and out of your lungs. Mechanical ventilation is the use of a machine to move air in and out of your lungs.
Do they intubate you while awake?
Usually this tube is inserted after you are asleep. Awake Fibreoptic Intubation (AFOI) is when a breathing tube is placed in the breathing passage through the nose or the mouth when you are awake.
Are you intubated for a colonoscopy?
You won’t be completely unconscious, but you’ll sleep through the procedure and probably have no memory of it. The medication commonly used for deep sedation is propofol, which is not an opioid. It acts fast, wears off quickly, and is safe for most patients.
What can I use instead of succinylcholine?
Rocuronium, introduced more recently for use in emergency situations, has been proposed as a good alternative to succinylcholine because of its pharmacokinetic characteristics. When used at a dose of 1.2 mg/kg, rocuronium has a similar onset time to succinylcholine.
What can I use in place of succinylcholine?
Traditionally succinylcholine has been the most commonly used muscle relaxant for this purpose because of its fast onset and short duration; unfortunately, it can have serious side effects. Rocuronium has been suggested as an alternative to succinylcholine for intubation.
Which drugs are used for treating rapid sequence intubation RSI )? Select all that apply?
- Ketamine 1.5-2 mg/kg IBW.
- Etomidate 0.3-0.4 mg/kg TBW.
- Fentanyl 2-10 mcg/kg TBW.
- Midazolam 0.1-0.3 mg/kg TBW.
- Propofol 1-2.5 mg/kg IBW + (0.4 x TBW) (others simply use 1.5 mg/kg x TBW as the general guide)
- Thiopental 3-5 mg/kg TBW.
Does being intubated hurt?
Intubation is an invasive procedure and can cause considerable discomfort. However, you’ll typically be given general anesthesia and a muscle relaxing medication so that you don’t feel any pain. With certain medical conditions, the procedure may need to be performed while a person is still awake.
Why is a trach better than a ventilator?
Tracheostomy is thought to provide several advantages over translaryngeal intubation in patients undergoing PMV, such as the promotion of oral hygiene and pulmonary toilet, improved patient comfort, decreased airway resistance, accelerated weaning from mechanical ventilation (MV) [4], the ability to transfer ventilator …
Is patient conscious on ventilator?
Most often patients are sleepy but conscious while they are on the ventilator—think of when your alarm clock goes off but you aren’t yet fully awake. Science has taught us that if we can avoid strong sedation in the ICU, it’ll help you heal faster.
How do they wake you up from propofol?
Recovery from propofol anesthesia may be sped up by use of common stimulant. Summary: The ability of the commonly used stimulant methylphenidate (Ritalin) to speed recovery from general anesthesia appears to apply both to the inhaled gas isoflurane, as previously reported, and to the intravenous drug propofol.
Is precedex better than propofol?
Conclusions: For ICU patient sedation, dexmedetomidine may offer advantages over propofol in terms of decrease in the length of ICU stay and the risk of delirium. However, transient hypertension may occur when dexmedetomidine is administered with a loading dose or at high infusion rates.
Can you take propofol and precedex together?
Using propofol together with dexmedetomidine may have increased effects on breathing, heart rate, blood pressure, and sedation. You will be monitored closely by your surgical team during anesthesia, and the doses of each medication adjusted accordingly.
Who should not be given propofol?
You should not receive propofol if you are allergic to it. To make sure propofol is safe for you, tell your doctor if you have: epilepsy or other seizure disorder; or. high cholesterol or triglycerides (a type of fat in the blood).
What is the 1 2 life of propofol?
Half-life: Propofol is bi-phasic, with its initial half-life being relatively quick, around 40 minutes, and its terminal half-life usually being 4 to 7 hours.
What drug category is propofol?
Propofol Overview Propofol belongs to a group of drugs called general anesthetics. These work by slowing activity in the brain to prevent pain and allow sleep.
WHO recommends against using remdesivir?
WHO has issued a conditional recommendation against the use of remdesivir in hospitalized patients, regardless of disease severity, as there is currently no evidence that remdesivir improves survival and other outcomes in these patients.
Is remdesivir bad?
WHO has a regular overview of possible adverse drug events related to COVID-19 treatments. In late August it noted a disproportionately high number of reports of liver and kidney problems in patients receiving remdesivir compared with patients receiving other drugs for COVID-19.
Is there oral remdesivir?
Remdesivir is an antiviral approved for COVID-19 treatment, but its wider use is limited by intravenous delivery. An orally bioavailable remdesivir analog may boost therapeutic benefit by facilitating early administration to non-hospitalized patients.
Does a ventilator damage your lungs?
Ventilator Complications: Lung Damage If the force or amount of air is too much, or if your lungs are too weak, it can damage your lung tissue. Your doctor might call this ventilator-associated lung injury (VALI).
Do you gag when intubated?
Traditionally, the presence of a gag reflex has been used to guide intubation decisions. A weak gag reflex is an important risk factor for aspiration pneumonia, so its absence may trigger intubation in at-risk patients. The absence of a gag reflex may also suggest brain death in comatose patients.
What happens when you wake up intubated?
Awake intubation is placing an endotracheal tube in the trachea while the patient continues to breathe. The principle advantage over RSI is that you do not take away the patient’s respirations or airway reflexes, which makes the process safer in many circumstances.
